
Hormone testing for women often starts at a frustrating moment. A woman may be tracking cycles, trying to conceive, noticing mood changes, spotting, fatigue, or PMS that feels different than usual, and wondering whether lab work will finally provide answers.
That question is reasonable. Hormones affect ovulation, the uterine lining, energy, sleep, stress response, thyroid function, and fertility planning. But hormone testing doesn’t work like a simple pass-or-fail quiz. A result only becomes meaningful when it matches the right test, the right timing, and the right clinical question.
More than 80% of women report hormone-related symptoms, like hot flashes and night sweats, at some point in life, which helps explain why fertility and cycle workups often include markers such as estradiol, progesterone, LH, FSH, testosterone, DHEA-S, SHBG, prolactin, cortisol, and thyroid hormones, with sex hormones often checked in the mid-luteal phase, days 19 to 21 of a 28-day cycle, while some other markers can be tested at any time.
Understanding the Key Hormones for Your Fertility
Fertility hormones work more like an orchestra than a row of isolated switches. If one section is too quiet, too loud, or coming in at the wrong time, the whole performance can feel off. That is why a fertility panel usually looks at several hormones together instead of chasing one number.
The hormones that help tell the fertility story
A useful way to think about these hormones is in terms of their job descriptions.
- FSH and LH: These are messengers from the brain to the ovaries. FSH helps recruit and mature follicles. LH helps trigger ovulation. If either signal is out of step, ovulation can become irregular or fail to occur as expected.
- Estradiol: The main estrogen during the reproductive years. It helps build the uterine lining and reflects what the developing follicles are doing.
- Progesterone: After ovulation, progesterone prepares the uterus for possible implantation. In plain language, it helps turn a freshly built lining into one that can support an embryo.
- AMH: This marker is often used as part of an ovarian reserve discussion. It can be helpful in planning, but it should never be treated as a crystal ball.
- Prolactin, testosterone, DHEA-S, SHBG, cortisol, and thyroid hormones: These aren’t side characters. They can influence cycle regularity, ovulation, mood, energy, metabolism, and fertility.
A hormone result matters most when it answers a specific question, such as “Did ovulation likely happen?” or “Could a thyroid issue be affecting cycles?”
Why one result rarely tells the whole story
Readers often get stuck here. A woman may hear that one hormone is “normal” and assume everything is fine, or hear that one value is off and assume the entire fertility picture is poor. Neither conclusion is always accurate.
Hormones change across the cycle. They also influence one another. A progesterone value, for example, means far more when the timing of ovulation is known. Thyroid markers may matter even if periods are still arriving every month. Androgen-related markers may be relevant when acne, hair changes, or long cycles are present.
A simple mental model can help:
| Hormone group | What can it help clarify |
| Cycle regulators | Whether the brain and ovaries are coordinating well |
| Ovulation markers | Whether an egg is likely to be released, and the luteal phase looks active |
| Reserve markers | Planning questions, especially when fertility treatment is being considered |
| Whole-body hormones | Whether thyroid, stress, or prolactin patterns may be affecting fertility |
A fertility workup is usually strongest when symptoms and labs are read together. A woman with regular cycles but recurrent PMS, spotting, or trouble conceiving may need a different testing strategy than someone with very unpredictable periods.
A lab panel is a map, not the destination. It helps show where to look next.
Your Guide to Hormone Testing for Women
The logistics of hormone testing for women confuse many patients more than the blood draw itself. The same hormone can look completely different depending on when it was tested and how the sample was collected.
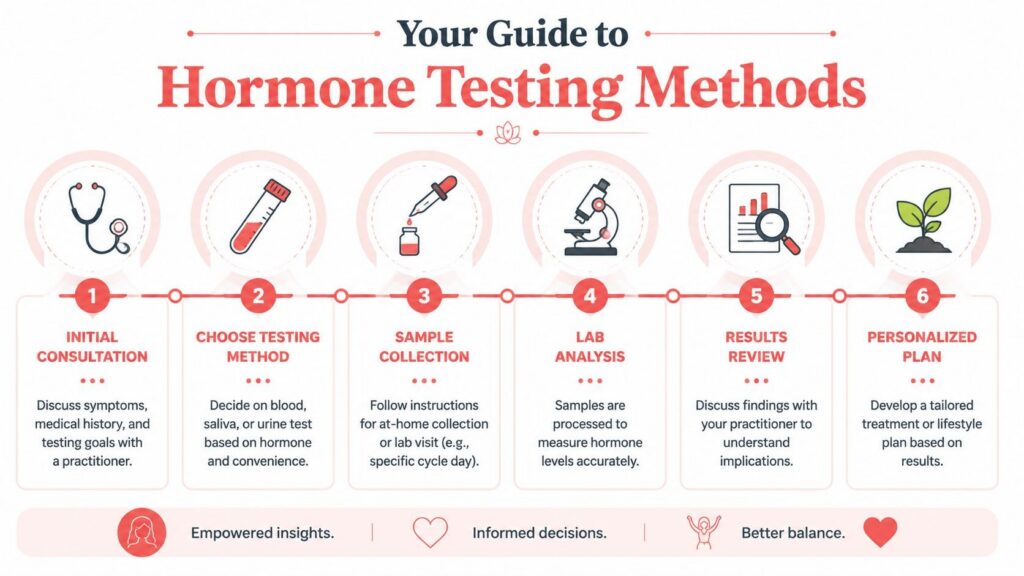
The main testing methods
| Method | Often used for | Main point to remember |
| Blood or serum testing | Gonadotropins, thyroid markers, prolactin, and reproductive hormones | This is the standard approach for many fertility questions |
| Saliva testing | Repeated sampling across the cycle in some panels | It may help show patterns over time rather than a single moment |
| Urine testing | Repeated daily measurements or a longer collection window | It can be useful when the goal is to track changing hormone output |
Clinical guidance notes that the choice of test should match the question being asked. Serum is standard for many reproductive and thyroid tests. Saliva panels may use 1 to 11 saliva samples across the cycle to characterize cyclic variation, and urine testing can be useful when repeated measurements are needed, especially when symptoms suggest hormone swings rather than a steady-state problem.
Why timing changes everything
Timing is not a minor detail. It is the difference between a helpful answer and a misleading one.
Clinical guidance emphasizes that the common day 21 progesterone test is really a shortcut. The more accurate recommendation is to measure progesterone 7 days before the expected onset of menses. The same guidance notes that a luteal progesterone level below 20 nmol/L suggests ovulation is unlikely. In contrast, a level above 30 nmol/L strongly suggests ovulation when the test is performed at the correct time, according to this clinical review on progesterone timing and ovulation assessment.
That matters because not every woman ovulates on the same calendar day. A woman with a longer cycle may ovulate later. A woman with an irregular cycle may need more than one progesterone measurement. For that reason, fixed-date testing can create confusion.
A helpful example:
- Regular cycle: If periods arrive predictably, the clinician can estimate the likely luteal testing window more accurately.
- Irregular cycle: Testing may need to follow symptoms, signs of ovulation, or repeated sampling rather than a standard calendar rule.
- Trying to confirm ovulation: The question isn’t only “What is the progesterone number?” It’s also “Was this drawn at the right time?”
For readers trying to understand whether ovulation is even happening, this guide on how to know if ovulation is occurring can help connect timing, symptoms, and testing.
Making Sense of Your Hormone Test Results
A lab report can feel deceptively precise. There are columns, reference ranges, and flagged values. Yet fertility interpretation is usually more nuanced than a red arrow next to one number.
Patterns that may point the conversation in a direction
Certain patterns of results may help a clinician decide what to investigate next. They are clues, not self-diagnoses.
A few common examples:
- Irregular or absent ovulation patterns: If progesterone doesn’t align with the expected post-ovulation window, the question may be whether ovulation occurred or whether the sample was taken at the wrong time.
- PCOS-type patterns: Some women show a pattern of irregular cycles, signs of higher androgens, or ovulation issues that may fit a broader PCOS picture. That interpretation should always be paired with symptoms and history, not a lab value alone.
- Thyroid-related concerns: A woman may be focused on fertility, while the bigger issue is that thyroid imbalance is disrupting cycle regularity, energy, or ovulation.
- Perimenopausal transition: Fluctuating hormone levels can make test results harder to interpret. In that setting, symptoms and cycle history become especially important.
For women navigating irregular cycles or suspected androgen-related symptoms, this PCOS overview may help frame which lab findings deserve a more careful conversation.
Numbers can suggest a direction. They don’t replace clinical judgment.
Questions worth asking after a lab report
Many patients feel pressure to understand everything immediately. A better approach is to ask better questions.
| Question to ask | Why it matters |
| Was this test drawn at the right point in the cycle? | Timing can change the interpretation completely |
| Does this result match the symptoms? | A value that looks acceptable on paper may still not answer the real concern |
| Is this a single snapshot, or does repeat testing make sense? | Some patterns only appear when levels are followed over time |
| Does this change treatment or planning? | Not every abnormality needs the same response |
A woman trying to conceive may also want to ask whether the result affects her plans for natural conception, fertility treatment, or follow-up observation. Those are not the same thing.
One more point often gets missed. More testing isn’t always better. A broad panel can create a pile of mildly interesting information that doesn’t clarify next steps. A focused panel tied to a symptom pattern is often more useful than a larger panel collected without a clear reason.
How Acupuncture May Support Your Hormonal Balance
Once lab results arrive, many women ask a practical question. What can be done with this information?
Western testing can identify patterns. Traditional Chinese Medicine looks at how those patterns are showing up in the body as a whole. That includes the menstrual cycle, sleep, digestion, emotional stress, temperature patterns, pain, and energy, not just the lab sheet.

How Traditional Chinese Medicine reads the bigger picture
In Traditional Chinese Medicine, a hormone imbalance isn’t viewed as one isolated chemical mistake. It may reflect a broader pattern of imbalance involving Qi, Blood, Yin, and Yang.
A woman with irregular cycles and stress-related PMS may not present the same way as a woman with scanty periods, fatigue, and signs of depletion, even if both are concerned about ovulation. In a TCM framework, one pattern may look more like stagnation, while another may look more like deficiency.
That matters because support is meant to match the pattern, not just the label on the chart.
A lab value may say “low progesterone.” A TCM assessment asks why the body may not be building and sustaining the second half of the cycle well.
What support may look like in practice
An acupuncture-based plan may include several layers:
- Acupuncture sessions: Often used to support cycle regulation, stress response, and overall reproductive balance.
- Lifestyle guidance: Sleep, meals, exercise intensity, and stress load can all affect how stable a cycle feels from month to month.
- Herbal or supplement discussions: These should be individualized, especially for anyone trying to conceive or working with a fertility clinic.
- Coordination with medical care: If a woman is doing an infertility workup, preparing for IVF, or managing PCOS, acupuncture should complement that care rather than replace it.
For readers seeking a deeper look at this integrative approach, this natural guide to acupuncture for hormonal imbalance explains how symptom patterns and root-cause thinking work together.
What to Expect at Your Longevity Acupuncture Consultation
A fertility-focused consultation should feel less like a rushed review of numbers and more like a careful reconstruction of the cycle story. The lab report matters, but it is only one chapter.
A consultation that looks beyond the lab slip
At an initial visit, the conversation usually includes cycle length, bleeding pattern, PMS, cervical mucus changes, basal body temperature if tracked, sleep, digestion, energy, stress, and fertility goals. If a woman is preparing for natural conception, IUI, or IVF, those details shape the plan differently.
Dr. Vivian Shou-Litman is a Florida-licensed acupuncture physician and NCCAOM Diplomate of Oriental Medicine. In a fertility setting, that means the discussion can bridge two languages at once. The language of lab markers and the language of whole-body pattern recognition.
How a plan gets personalized
A personalized plan may use hormone testing as a reference point rather than the sole target. For example:
- If timing is the issue: The plan may focus on cycle tracking and ovulation support.
- If stress appears to be amplifying symptoms, the plan may place greater emphasis on nervous system regulation and recovery.
- If cycles are irregular: The treatment rhythm may follow the woman’s actual cycle pattern rather than a textbook calendar.
- If fertility treatment is already underway: The acupuncture schedule may be coordinated around monitoring, retrieval, transfer, or luteal phase support.
In South Miami, Coral Gables, Pinecrest, Coconut Grove, and the wider South Florida area, some patients choose a clinic such as Longevity Acupuncture when they want fertility acupuncture integrated with lab review, cycle awareness, and a root-cause lens. The aim isn’t to chase a perfect spreadsheet. It’s to support a healthier, more coherent cycle in a way that fits the woman’s goals.
Common Questions About Hormone Testing
| Question | Answer Summary |
| Do women need every hormone tested at once? | Usually not. Focused testing tied to symptoms and fertility goals is often more useful than a broad panel without a clear question. |
| Are at-home hormone kits enough for fertility concerns? | They may be a starting point, but they often don’t replace clinical interpretation or standard blood-based testing. |
| Can hormone tests confirm ovulation by themselves? | They can help, especially when timed correctly, but the answer depends on the marker and the cycle day. |
| If results are normal, does that rule out a hormone problem? | Not necessarily. Symptoms, timing, and repeat testing may still matter. |
| How often should hormones be retested? | That depends on the original concern, whether treatment has started, and whether the results would change the next steps. |
One of the most common questions is whether a woman should order a large panel just to be safe. Often, that creates more noise than clarity. A better starting point is to identify the specific issue. Is the concern irregular periods, suspected lack of ovulation, recurrent PMS, possible PCOS, thyroid symptoms, or fertility planning before IVF?
Another frequent question involves at-home testing. Convenience is real, but limits matter too. Clinical guidance notes that at-home hormone kits are available, including fertility and thyroid options, yet blood-based testing and symptom-linked interpretation remain central for diagnosing infertility, PCOS, menopause, and ovulatory problems. The same guidance also notes that AMH can be useful for ovarian reserve. Still, it does not by itself predict natural conception, and broader panels may create confusion without changing management, according to this review of hormone testing options for women.
If a test result won’t change the next clinical decision, it may not be the right test to order first.
Referral questions come up often, too. Some women start with a primary care doctor or a gynecologist. Others begin with a fertility specialist because the main issue is conception. Women using complementary care may also bring prior lab work to an acupuncture consultation so the treatment plan can reflect both symptoms and existing medical evaluation.
A final point is worth keeping in mind. Hormone testing for women is most helpful when it serves a decision. That decision might be to confirm ovulation, clarify why cycles are irregular, decide whether thyroid follow-up is needed, or plan the next fertility step with more confidence.
For women in Miami and nearby South Florida communities who want help connecting lab results to cycle symptoms, fertility goals, and a whole-body treatment plan, Longevity Acupuncture offers consultations that integrate Traditional Chinese Medicine with thoughtful, personalized hormone testing.